We Were Sent Home From the Hospital with Instructions that Could Have Killed Our Son

I've just spent over five hours at the Summerlin Pediatrics ER here in Las Vegas, Nevada. Starting with our primary Doctor assuring me that my six-month-old son will be fine as I tear up after being told I need to take him to the ER for testing, its been a day with a range of emotions. At this point, I'm tired, grateful but angry.
The day was wrought with loads of crying (not just me), ultrasounds, tubes stuck in my son's penis (both of us crying), and needles. But that's not what I'm angry about.
I'm actually grateful that (as of now) all the tests, including intussusception (the reason we were sent to the ER) came back negative and it was decided that our son likely has a virus that needs to work its course.
I'm angry, however, that we were sent home with documentation on how to kill our son.
Well, that may be a bit dramatic...
We were sent home with dosage instructions that were calculated wrong and if we simply trusted the hospital and administered them as written, our son could have been seriously harmed and we would have ended up right back at the ER with another $1,500 visit copay.
Yes, our copay for the visit was a WHOPPING $1,500 but I'm not going to rant on how insane that is in this blog post. Back to the post at hand...
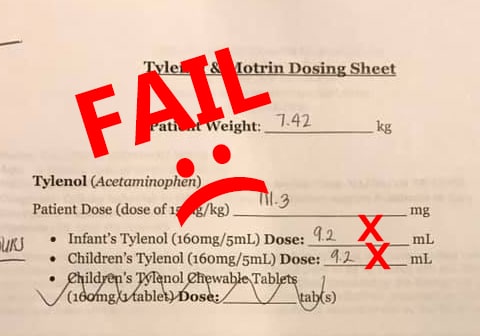
Below is the dosage instruction sheet we were sent home with:
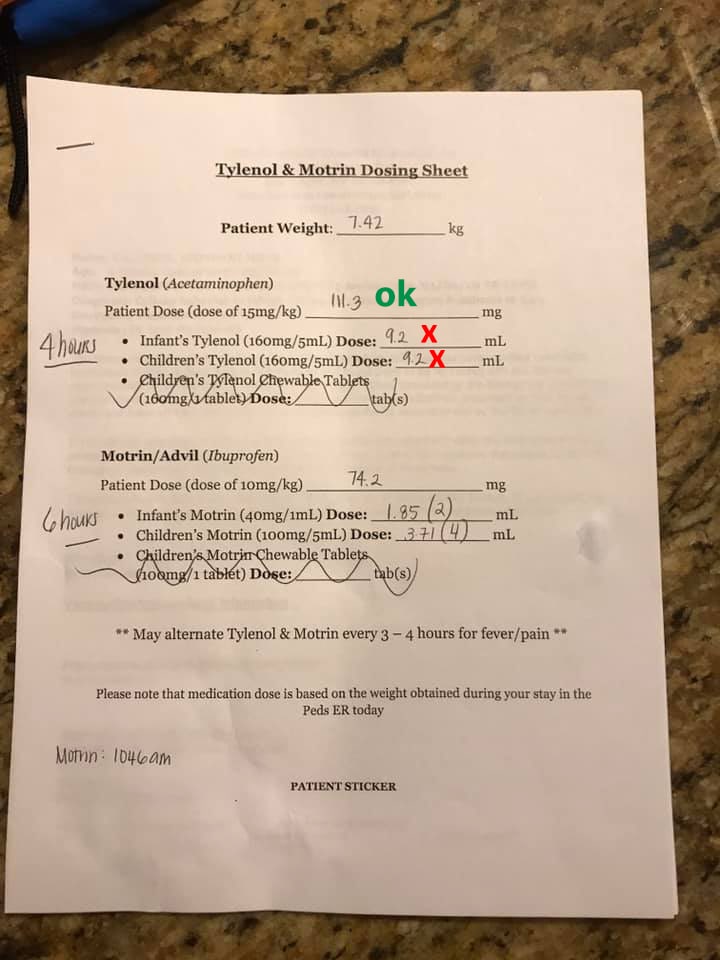
The "Patient Dose" is calculated to be 111.3mg of Tylenol, which was correctly computed based on our son's weight.
But the dosage was calculated incorrectly.
Take a look at the "Dose" for "Infant's Tylenol" and "Children's Tylenol". The amount is 9.2mL for both.
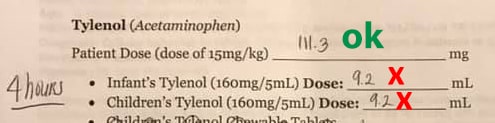
To quickly understand the calculation issue, notice that both formulations are 160mg/5mL. This means that if you give a child 5mL of either medicine, you are administering 160mg of Tylenol.
So 5mL, which is 160mg of Tylenol, is already greater than the 111.3mg of proper dosage.
But the nurse accidentally calculated an even higher amount 9.2mL of formulation to administer. If you do the math, this turns out to be 294.4mg of Tylenol. That's nearly 3 TIMES the proper dosage!
And remember... this isn't one particular individual dose that would be wrong... its an overdose that is stated to be given every four hours!
I can't readily find an official percentage that is considered a deadly overdose as most articles, like this one, just use the generic terms like "large" or "excessive" without actually defining what constitutes "large" or "excessive". However, even if 3x the recommended dose isn't "excessive", according to this Time Magazine article, "Study: Taking Just a Little Too Much Tylenol Each Time Can Be Deadly", even just a "little too much" can be deadly.
Interestingly during our visit, the ER doctor gave us a long talk about the dangers of overdosing on Tylenol. He told us about how it was so potent that people often commit suicide by taking extremely large dosages.
And he also told us a story (House, M.D style) of having to discover a child's trip to the ER was traced back to a parent accidentally overdosing the child with Tylenol.
So, of course, it's therefore fitting that the hospital sent us home with instructions for administering a dosage that could seriously harm or possibly even kill our child.
The mistake was caused because this informational sheet is manually calculated. Manual calculation is prone to errors because people, no matter how good they are at their jobs, make mistakes.
I am a technology consultant, so this is where my consultant's brain kicks in.
I don't blame the nurse that filled out the sheet for her mistake.
It's the hospital's mistake for not having either the right tool or a process in place to catch the error.
In the most simple case, there should at least be a process in place to make sure that if this mistake does happen, it will be caught. That remedy is to simply include on the sheet, a space for the nurse AND another staff member to initial that it was calculated by the nurse and reviewed by a second person.
But really this mistake shouldn't be possible to make!
The real mistake is that this sheet isn't auto-calculated.
The document is likely a Microsoft Word doc that the nurse prints out and fills in. It shouldn't be an MS Word doc. If not a simple internal application (that would be fairly inexpensive to create) it should at least be a Microsoft Excel spreadsheet where the nurse only has to enter the child's weight and the rest of the fields are auto-calculated.
Ultimately I'm blown away that as I recall watching the nurse go through the hospital's rigorous process of steps with scanning, counting, weighing, typing and re-typing when she herself was administering medicine to my son, but that same hospital would allow her to send us home with an unverified, hand calculated and therefore prone to error piece of information.
Obviously, for the potential safety of others, I will be contacting the hospital and make sure they know about and resolve this situation.
And I should note that the Doctor and Nurse were both wonderful, amazing people with fantastic bed-side manner. I am not upset at all with the care my son received while in the ER. I'm just blown away that this very simple potential for error still exists in a prominent hospital.
On a lighter note, my original title for this article was "The day our son cried himself immediately past triage and directly to the ER Dr".
Not really a great title.
My wife's idea was much funnier...
"The Day Our Son cried Gimself Into a $1,500 ER Visit Copay"
Leave a Reply
Recent Posts

Reolink Argus 2 Review: From an Owners Perspective
I Made the World a Little Safer!

A Typical Parenting Moment from the Parent of a Child with FASD

Volunteering
We Were Sent Home From the Hospital with Instructions that Could Have Killed Our Son
After School Programs: Your Child May Not Be As Safe As You Think

FAS - You Wouldn't Say That About My Child If It Was Autism

VicTsing Filterless Cool-Vapor Humidifier Review
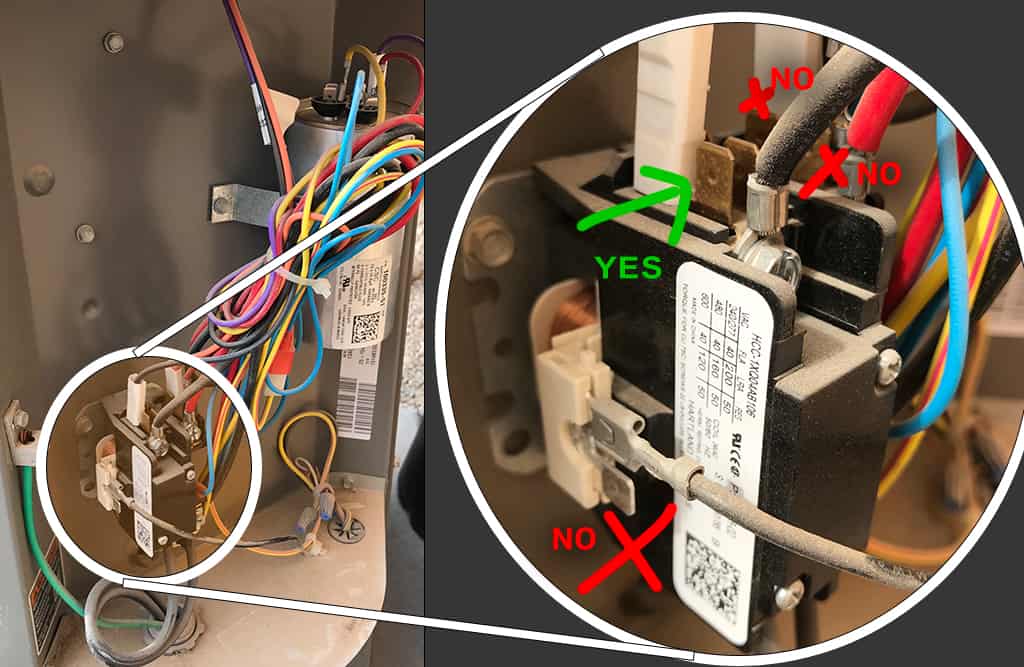
Increasing the Life of Your Air Conditioner: How to Install a 'Hard Start' Kit
A/C Hard Start Kit: A $1,600 Per Hour Story